Other treatments for achalasia include laparoscopic Hellers myotomy, pneumatic dilation, and botulinum injection. Please see below for a more detailed summary.
Laparoscopic Hellers Myotomy
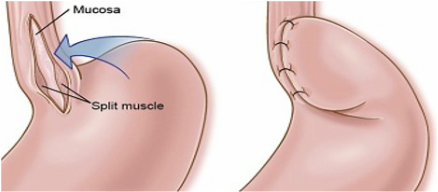
With the Laparoscopic Hellers myotomy, 4-5 small incisions are made in the skin and allows access to the abdominal organs. These incisions function as ports for various instruments. The esophagus and stomach are identified and are separated from the surrounding connective tissue. Once the esophagus has been adequately freed up, approximately 6-8 cm of the esophageal muscle is cut extending down to 2-3 cm to the stomach. Due to the disruption of the natural connections with the esophagus and surrounding structures, there is a high rate of reflux and an anti-reflux procedure is required. Specifically, the stomach is partially wrapped around the esophagus and sewn into place to reinforce the natural barrier to reflux.
Adverse events with Laparoscopic Heller's
Limitations of Laparoscopic Heller's
- Tears to mucosa during myotomy ~12% (Usually repaired immediately without clinical consequences)
- Reflux ~15% (highly variable)
- Bleeding (rare)
- Damage to the lung, spleen, stomach, esophagus or liver, or problems (very rare)
Limitations of Laparoscopic Heller's
- Treatment limited to Gastroesophageal junction
- Requirement for anti-reflux procedure due to very high rate of reflux without it
- For failed procedures/recurrent symptoms, re-operation is more complicated
- Patients generally require two weeks off from work
Pneumatic Dilation
For many years, repeated endoscopic pneumatic dilation was the treatment of choice, due to the the fact that the procedure is quick and easy to perform. In 2011, a trial published in the New England Journal of Medicine comparing pneumatic dilation to Laparsocopic Hellers Myotomy. They found that after 2 years follow-up there was no difference in success rates between the two treatments, both achieving success of over 85%. With a perforation rate of 4% for pneumatic dilation and tears in the mucosa in 12% of Heller myotomy patients.
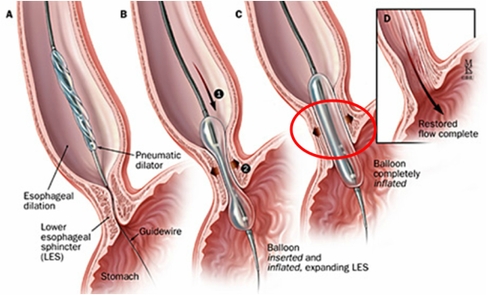
The pneumatic dilation procedure is generally as follows (see figure below):
The pneumatic dilation procedure is generally as follows (see figure below):
- An endoscopy of the upper GI tract is performed.
- A balloon is inserted over a guide wire and positioned across the junction of the esophagus and stomach
- Under X-ray, the balloon is inflated until the tight area at the junction is "opened up"
Adverse events with Pneumatic Dilation
Limitations of Pneumatic Dilation
- Perforation ~5%
- Reflux ~10-15%
- Chest pain (usually resolves within days)
- Bleeding (rare)
Limitations of Pneumatic Dilation
- Treatment limited to Gastroesophageal junction (Circled in figure)
- Patients usually require multiple dilation's
- Poor results with advanced achalasia
Botulinum (Botox) Injection
Usually 100 units of Botox is injected in 4 divided doses into the four quadrants of the lower esophageal sphincter, under direct vision. It is a safe procedure, with very few side effects or complications. The efficacy is approximately about 85% in the short-term, however, this decreases to 50% at six months and 30% after one year. In addition, repeat injections are generally less effective. Due to the poor long-term efficacy, this treatment is generally reserved for patients that are too unwell to undergo any of the other procedures.

Adverse events with Botox Injection
Limitations of Botox Injection
- Mucosal injury
- Bleeding (very rare)
- Non-fatal mediastinitis (infection in chest cavity) (very rare)
- Pneumothorax ( is an abnormal collection of air around the lung) (very rare)
Limitations of Botox Injection
- Treatment limited to Gastroesophageal junction
- Repeated injection can make other treatments more difficult
- About 70% of patients will have recurrence of symptoms within a year